Supporting Fact Library Graphics
Diagnosis
Note: This section contains facts for four groups: Children (ages 0-14), Children and Adolescents (ages 0-19), Adolescents (ages 15-19), Adolescents and Young Adults (Ages 15-39)
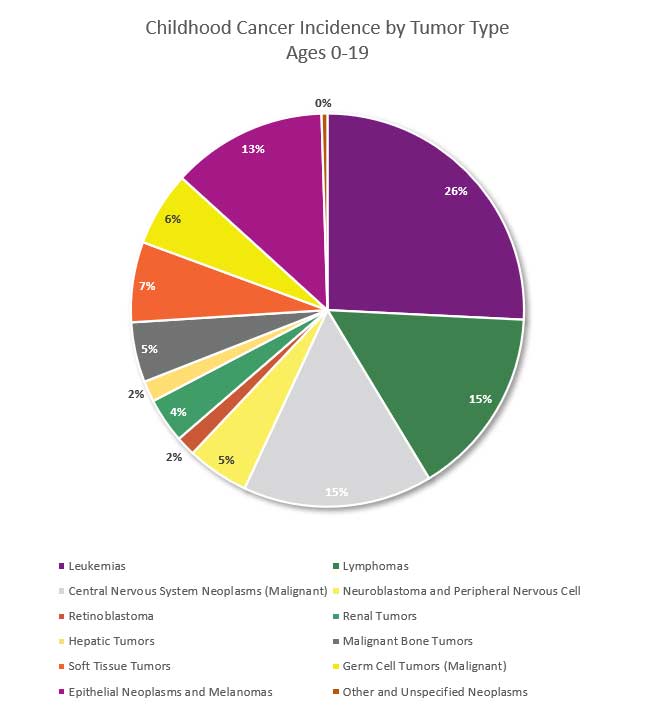
Figure Reference. NCCR*Explorer: An interactive website for NCCR cancer statistics [Internet]. National Cancer Institute; 2025 Sep 24. [cited 2026 Mar 26]. Available from: https://nccrexplorer.ccdi.cancer.gov.
- Childhood and Adolescent cancer (ages 0-19) is not one disease - there are more than 13 major types of pediatric cancers and over 200 subtypes.1 Paediatric Tumours. 5th edn, Vol. 7 (International Agency for Research on Cancer, 2023).
- One in 264 children & adolescents is estimated to be diagnosed with cancer before the age of 20 years.2 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- The average age at diagnosis is 10 overall (ages 0 to 19), 6 years old for children (aged 0 to 14), and 17 years old for adolescents (aged 15 to 19)3 Howlander, N. et al. SEER Cancer Statistics Review, 1975-2018, https://seer.cancer.gov/archive/csr/1975_2018/ (2021). , while adults’ median age for cancer diagnosis is 66.4 National Cancer Institute. Age and Cancer Risk, https://www.cancer.gov/about-cancer/causes-prevention/risk/age (2024).
- Leukemia is the most common childhood cancer (ages 0-14), accounting for 28% of cases, followed closely by central nervous system tumors (27%), one-third of which are benign or borderline malignant. In adolescents (ages 15-19), the most common cancer is central nervous system tumors (22%), more than one-half of which are benign or borderline malignant, followed by lymphoma (19%) and leukemia (13%).5 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- After increasing since at least 1975, the overall invasive cancer incidence rate in children (ages 0-14), declined slightly from 2015 through 2021 by 0.8% per year driven by a recent rapid decline in malignant brain tumors (from 37.3 per million in 2017 to 31.9 per million in 2021) and stabilized rates of lymphoid leukemia. In contrast, overall incidence continued a slow increase in adolescents (by 0.7% per year) because of climbing rates for both lymphoid leukemia and non-Hodgkin lymphoma. Malignant brain tumors decreased rapidly, consistent with the pattern in children, but represent only 9% of all malignancies versus 20% in children.6Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10-45. doi:10.3322/caac.21871
- In 2025, an estimated 9550 children (aged birth to 14 years) and 5140 adolescents (aged 15–19 years) will be diagnosed with cancer.7 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- Approximately 5.7% of newly diagnosed brain tumors, including adults, occur under age 20.8 Ostrom, Q. T. et al. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2015–2019. Neuro-Oncology 24, v1–v95 (2022). https://doi.org/10.1093/neuonc/noac202
- Childhood brain and other nervous system cancers are most frequently diagnosed among ages 5–9.9Cancer Stat Facts: Childhood Brain and Other Nervous System Cancer (Ages 0–19). SEER 12. Published online 2024. https://seer.cancer.gov/statfacts/html/childbrain.html
- Children with Down syndrome have a 20-fold increased risk of acute lymphoblastic leukaemia (ALL), and nearly a 500-fold increased risk of acute myeloid leukaemia (AML) before the age of 5.10 Wachtmeister, A. et al. Lifetime risk of solid tumors and leukemia in Down Syndrome: a population-based Swedish matched cohort study. British Journal of Cancer 134, 790–798 (2026). https://doi.org/10.1038/s41416-025-03318-5
- Pediatric head and neck tumor diagnoses have been on the rise and more commonly affect females. These tumors appear in a bimodal distribution; they most commonly present in very young patients and then during late adolescence. The incidence has increased since 2000, and faster than overall incidence.11 Kraguljac, S., Hajjar, F., Wong, R., Shah, J. & Lopez, J. Pediatric Head and Neck Malignancies in the United States: A 20‐Year Population‐Based Study. Pediatric Blood & Cancer 72 (2025). https://doi.org/10.1002/pbc.31452
First time Cancer Diagnosis for Adolescents and Young Adults (AYA’s) Ages 15 to 39
- In 2025, it is estimated that there will be 85,480 new cases of cancer among AYAs in the United States.12 National Cancer Institute. Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15–39), https://seer.cancer.gov/statfacts/html/aya.html (2024).
- Overall cancer incidence rates for AYAs increased an average of 0.3% per year between 2013 and 2022. Death rates have been falling 0.9% each year, on average, over the same time period in the United States.13 National Cancer Institute. Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15–39), https://seer.cancer.gov/statfacts/html/aya.html (2024).
- Globally, the most common cancers among AYAs are breast, thyroid, and cervical, while the leading causes of death are breast, cervical, and leukemia. While incidence is higher in countries with a higher Human Development Index (HDI), those with lower HDI face disproportionately higher mortality.14 Li, W. et al. Global cancer statistics for adolescents and young adults: population based study. Journal of Hematology & Oncology 17 (2024). https://doi.org/10.1186/s13045-024-01623-9
Survival
- Cancer survival rates vary not only depending on the type of cancer, but also on individual factors attributable to each child.15 Smith, M. A. et al. Outcomes for Children and Adolescents With Cancer: Challenges for the Twenty-First Century. Journal of Clinical Oncology 28, 2625–2634 (2010). https://doi.org/10.1200/jco.2009.27.0421 Five-year survival rates can range from almost 0% for cancers such as DIPG (2.2%), a type of brain cancer16 Hoffman, L. M. et al. Clinical, Radiologic, Pathologic, and Molecular Characteristics of Long-Term Survivors of Diffuse Intrinsic Pontine Glioma (DIPG): A Collaborative Report From the International and European Society for Pediatric Oncology DIPG Registries. Journal of Clinical Oncology 36, 1963–1972 (2018). https://doi.org/10.1200/jco.2017.75.9308 , to over 90% for the most common type of childhood cancer known as Acute Lymphoma Leukemia (ALL).17 Surveillance Research Program, National Cancer Institute (2025).
- The average 5-year survival rate for childhood cancer (Ages 0-19) as a whole is 86%.18 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- The most common severe or life-threatening chronic health problems related to childhood cancer or its treatment are endocrine disorders such as hypothyroidism or growth hormone deficiency (44%), subsequent neoplasms such as breast cancer or thyroid cancer (7%), and cardiovascular disease such as cardiomyopathy or congestive heart failure, coronary artery disease, and cerebrovascular disease (5.3%).19 Bhatia, S., Tonorezos, E. S. & Landier, W. Clinical Care for People Who Survive Childhood Cancer. JAMA 330, 1175 (2023). https://doi.org/10.1001/jama.2023.16875
- Individuals at highest risk for developing treatment-related health problems include patients with brain cancer treated with cranial irradiation (approximately 70% develop severe or life-threatening health problems) and allogeneic hematopoietic stem cell transplant recipients (approximately 60% develop severe or life-threatening health problems).20 Bhatia, S., Tonorezos, E. S. & Landier, W. Clinical Care for People Who Survive Childhood Cancer. JAMA 330, 1175 (2023). https://doi.org/10.1001/jama.2023.16875
- Individuals at the lowest risk for developing treatment-related health problems include those who survived solid tumors (such as Wilms tumor) treated with surgical resection alone or with minimal chemotherapy, for whom the prevalence of subsequent health problems is similar to people who did not have cancer during childhood or adolescence.21 Bhatia, S., Tonorezos, E. S. & Landier, W. Clinical Care for People Who Survive Childhood Cancer. JAMA 330, 1175 (2023). https://doi.org/10.1001/jama.2023.16875
- Diffuse Intrinsic Pontine Glioma (DIPG) represents approximately 80% of the malignant brainstem tumors occurring in children.22 Pai Panandiker, A. S. et al. Effect of time from diagnosis to start of radiotherapy on children with diffuse intrinsic pontine glioma. Pediatric Blood & Cancer 61, 1180–1183 (2014). https://doi.org/10.1002/pbc.24971 In the United States, about 300 children are diagnosed with DIPG each year. DIPG primarily affects children between the ages of 5 and 10 years, but can occur in younger children and teens. DIPG is rare in adults.23 National Cancer Institute. Cancer Stat Facts: Childhood Brain and Other Nervous System Cancer (Ages 0–19), https://seer.cancer.gov/statfacts/html/childbrain.html (2024).
- Despite numerous clinical trials, outcomes of children with DIPG continues to remain dismal, with a median survival of only 11 months, while only 10% of DIPG patients have a ≥ 2-year overall survival (OS) rate.24 Hoffman, L. M. et al. Clinical, Radiologic, Pathologic, and Molecular Characteristics of Long-Term Survivors of Diffuse Intrinsic Pontine Glioma (DIPG): A Collaborative Report From the International and European Society for Pediatric Oncology DIPG Registries. Journal of Clinical Oncology 36, 1963–1972 (2018). https://doi.org/10.1200/jco.2017.75.9308
- As of 2022, more than 521,000 pediatric cancer survivors were living in the United States, a number projected to exceed 580,000 by 2040.25 Primm, K. M., Blackman, E., Sansbury, B. M., Zaidi, S. K. & Sengupta, R. AACR Pediatric Cancer Progress Report 2025. Clinical Cancer Research 32, 465–467 (2026). https://doi.org/10.1158/1078-0432.ccr-25-4722
- There are more than 2.1 million cancer survivors diagnosed in the AYA period (ages 15-39) who are living in the United States; most are more than 10 years from diagnosis.26 Page, L. L. et al. Prevalence of cancer survivors diagnosed during adolescence and young adulthood in the United States. JNCI: Journal of the National Cancer Institute 117, 529–536 (2025). https://doi.org/10.1093/jnci/djae250
Pediatric Cancer 5-Year Relative Survival Percentage, Ages 0 to19 for years 2018 through 2022: The table below is a representation of the estimated 5-year survival rates for various types of childhood cancers. It should be noted that the survival rates listed below reflect general rates and are in no way a representation of an anticipated actual survival outcome for any individual child.27 NCCR*Explorer: An interactive website for NCCR cancer statistics [Internet]. National Cancer Institute; 2025 Sep 24. [cited 2026 Mar 26]. Available from: <a href=”https://nccrexplorer.ccdi.cancer.gov” target=”_blank” rel=”noopener noreferrer”>https://nccrexplorer.ccdi.cancer.gov</a>.
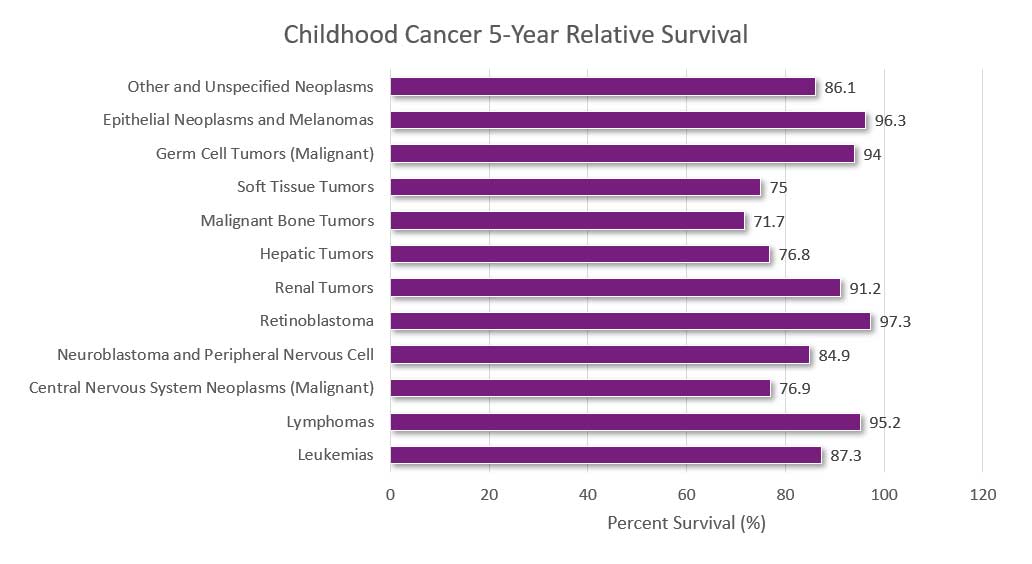
NCCR*Explorer: An interactive website for NCCR cancer statistics [Internet]. National Cancer Institute; 2025 Sep 24. [cited 2026 Mar 26]. Available from: https://nccrexplorer.ccdi.cancer.gov.
Long Term Health-Effects Associated with Treatments & Survival
- Cancer treatments may harm the body's organs, tissues, or bones and cause health problems later in life. They may include physical, mental, and social problems and second cancers. These health problems are called late effects as a result of surgery, chemotherapy, radiation therapy, and/or stem cell transplant. Late effects in childhood cancer survivors affect the body and mind. Late effects may affect organs, tissues, body function, growth and development. Other late effects are mood, feelings and actions thinking, learning, and memory as well as social and psychological adjustment. Late effects also have a risk of second cancers.28 National Cancer Institute. Late Effects of Treatment for Childhood Cancer (PDQ®)–Patient Version, https://www.cancer.gov/types/childhood-cancers/late-effects-pdq (2025).
- The chance of having late effects increases over time. New treatments for childhood cancer have decreased the number of deaths from the primary cancer. Because childhood cancer survivors are living longer, they are having more late effects after cancer treatment. Survivors may not live as long as people who did not have cancer.29 National Cancer Institute. Late Effects of Treatment for Childhood Cancer (PDQ®)–Patient Version, https://www.cancer.gov/types/childhood-cancers/late-effects-pdq (2025).
- Overall, children (ages 0-14) and adolescent and young adult (ages 15-39) cancer survivors were 57% more likely to develop depression, 29% more likely to develop anxiety, and 56% more likely to develop psychotic disorders in the years following treatment compared to their siblings or healthy members of a control group.30 Lee, A. R. Y. B. et al. Lifetime Burden of Psychological Symptoms, Disorders, and Suicide Due to Cancer in Childhood, Adolescent, and Young Adult Years. JAMA Pediatrics 177, 790 (2023). https://doi.org/10.1001/jamapediatrics.2023.2168
- Adult survivors of childhood cancer have a higher risk of developing cognitive impairment later in adulthood.31 Phillips, N. S. et al. Late-onset Cognitive Impairment and Modifiable Risk Factors in Adult Childhood Cancer Survivors. JAMA Network Open 6, e2316077 (2023). https://doi.org/10.1001/jamanetworkopen.2023.16077
- Childhood cancer survivors who received radiation or certain types of chemotherapy have an increased risk of late effects to the heart and blood vessels and related health problems.32 National Cancer Institute. Late Effects of Treatment for Childhood Cancer (PDQ®)–Patient Version, https://www.cancer.gov/types/childhood-cancers/late-effects-pdq (2025).
- NCI researchers observed that children who received radiotherapy had an increased risk of developing meningioma, cancer of the membranes that surround the brain and spinal cord meninges.33 Withrow, D. R. et al. Pooled Analysis of Meningioma Risk Following Treatment for Childhood Cancer. JAMA Oncology 8, 1756 (2022). https://doi.org/10.1001/jamaoncol.2022.4425
- Long-term survivors of childhood cancer are at substantially elevated risk of treatment-related adverse health effects as they age. For example, one longitudinal study found that 18% of childhood cancer survivors had experienced a major cardiovascular event by the age of 50 years compared with 0.9% of community controls. Thus, survivorship care plans are particularly critical for young survivors to help facilitate informed prevention and early detection interventions in addition to surveillance for subsequent cancers.34 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- Children and adolescents (ages 0 to 19) treated more recently, after 1986, may have lower risks of late effects due to modifications in treatment regimens to reduce exposure to radiotherapy and chemotherapy, increased efforts to detect late effects, and improvements in medical care for late effects.35 Ross, J. A., Spector, L. G., Robison, L. L. & Olshan, A. F. Epidemiology of leukemia in children with Down syndrome. Pediatric Blood & Cancer 44, 8–12 (2005). https://doi.org/10.1002/pbc.20165
- More than 95% of childhood cancer survivors will have a significant health-related issue by the time they are 45 years of age 36 Bhatia, S., Tonorezos, E. S. & Landier, W. Clinical Care for People Who Survive Childhood Cancer. JAMA 330, 1175 (2023). https://doi.org/10.1001/jama.2023.16875 ; these health-related issues are late effects of either the cancer or, more commonly, the result of its treatment. 1/3 will suffer severe and chronic side effects; 1/3 will suffer moderate to severe health problems; and 1/3 will suffer slight to moderate side effects.37 Hudson, M. M. et al. Clinical Ascertainment of Health Outcomes Among Adults Treated for Childhood Cancer. JAMA 309, 2371 (2013). https://doi.org/10.1001/jama.2013.6296
- Children and adolescent brain cancer survivors experience significant life-long morbidity from treatment. They have a higher incidence of chronic health conditions, including pulmonary fibrosis, cardiac dysfunction, endocrinopathies, neuropathies, and neurocognitive deficits.38 Rumberger Rivera, L. et al. Opportunities in the translational pipeline for pediatric brain cancer therapies. Pediatric Research 98, 800–806 (2025). https://doi.org/10.1038/s41390-025-03847-y
- Cognitive impairment affects up to one-third of childhood cancer survivors.39 Miller, K. D. et al. Cancer treatment and survivorship statistics, 2019. CA: A Cancer Journal for Clinicians 69, 363–385 (2019). https://doi.org/10.3322/caac.21565
- Long-term survivors of childhood cancer may be at elevated risk for new neurocognitive impairment and decline as they age into adulthood.40 Phillips, N. S. et al. Late-onset Cognitive Impairment and Modifiable Risk Factors in Adult Childhood Cancer Survivors. JAMA Network Open 6, e2316077 (2023). https://doi.org/10.1001/jamanetworkopen.2023.16077
- A large follow-up study of pediatric cancer survivors found that almost 10% developed a second cancer (most commonly female breast, thyroid, and bone) over the 30-year period after the initial diagnosis.41 Miller, K. D. et al. Cancer treatment and survivorship statistics, 2019. CA: A Cancer Journal for Clinicians 69, 363–385 (2019). https://doi.org/10.3322/caac.21565
- The reproductive system is particularly vulnerable to the negative impacts of cancer therapies. For example, alkylating agents and radiation can damage ovarian and testicular tissue, leading to fertility challenges, which impact childhood cancer survivors’ quality of life and mental health, and have been associated with depression, anxiety, and trauma. Assisted reproductive technologies provide viable fertility options, but early counseling and integrated reproductive care are essential to optimize outcomes for childhood cancer survivors. 42 Sorial, E. et al. Infertility, the outcomes of assisted reproductive technologies use in childhood cancer survivors: a scoping review. Journal of Cancer Survivorship (2026). https://doi.org/10.1007/s11764-026-01988-5
- Having a bone marrow or stem cell transplant usually involves receiving high doses of chemotherapy and sometimes radiation to the whole body before the procedure. In most cases, this permanently stops ovaries from releasing eggs, resulting in lifelong infertility.43 American Cancer Society. How Cancer and Cancer Treatment Can Affect Fertility in Women, https://www.cancer.org/cancer/managing-cancer/side-effects/fertility/how-cancer-treatments-affect-fertility-women.html (2025).
- Women treated with radiation therapy to the chest area for Hodgkin lymphoma at a young age have a 3-7 times higher risk of breast cancer than women who had Hodgkin lymphoma at a young age, but were not treated with radiation therapy.44 Ibrahim, E. M., Abouelkhair, K. M., Kazkaz, G. A., Elmasri, O. A. & Al-Foheidi, M. Risk of second breast cancer in female Hodgkin’s lymphoma survivors: a meta-analysis. BMC Cancer 12, 197 (2012). https://doi.org/10.1186/1471-2407-12-197
- Cardiovascular disease (CVD) in particular is a leading cause of mortality in survivors with increased risks for cardiac late effects. These late effects are attributable to the cardiotoxicities of cancer-related treatment. Complications from chemotherapeutics, for example, include hypertension, dyslipidemia, cardiomyopathy, valvular abnormalities, and coronary artery disease.45 Ackerman, A. et al. Long-Term Care of Childhood Cancer Survivors at Risk for Cardiac Late Effects. JACC: CardioOncology 7, 309–311 (2025). https://doi.org/10.1016/j.jaccao.2025.01.008
- Children who were treated for bone cancer, brain tumors, and Hodgkin lymphoma, or who received radiation to their chest, abdomen, or pelvis, have the highest risk of serious late effects from their cancer treatment, including second cancers, joint replacement, hearing loss, and congestive heart failure.46 National Cancer Institute. Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15–39), https://seer.cancer.gov/statfacts/html/aya.html (2024).
- Compared with the general population, survivors of childhood and adolescent cancers have an increased risk of 6 major psychiatric disorders, including: Autism spectrum disorder (hazard ratio [HR], 10.42), ADHD (HR, 6.59), PTSD (HR, 6.10), OCD (HR, 3.37), Major depressive disorder (HR, 1.88), Bipolar disorder (HR, 2.93).47 Hsu, T.-W. et al. Risk of Major Psychiatric Disorders Among Children and Adolescents Surviving Malignancies: A Nationwide Longitudinal Study. Journal of Clinical Oncology 41, 2054–2066 (2023). https://doi.org/10.1200/jco.22.01189
- Life expectancy for five-year childhood cancer survivors has steadily increased. Life expectancy for those treated in the 70’s is only 48.5 years and survivors treated in the 80’s have a life expectancy of 53.7 years, while those treated in the 90’s rose to 57.1 years.48 Bhatia, S., Tonorezos, E. S. & Landier, W. Clinical Care for People Who Survive Childhood Cancer. JAMA 330, 1175 (2023). https://doi.org/10.1001/jama.2023.16875 Normal life expectancy for adults is 77.5 years.49 Arias, E., Kochanek, K., Xu, J. & Tajeda-Vera, B. Provisional Life Expectancy Estimates for 2022. (National Center for Health Statistics, 2023).
- Nearly a quarter of childhood cancer survivors experience at least one debilitating neuromuscular condition 20 years post diagnosis.50 Rodwin, R. L. et al. Longitudinal Evaluation of Neuromuscular Dysfunction in Long-term Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study. Cancer Epidemiology, Biomarkers & Prevention 30, 1536–1545 (2021). https://doi.org/10.1158/1055-9965.epi-21-0154
- Nearly 30% of childhood cancer survivors developed pre-diabetes compared with less than 20% of patients in a matched control group. Further analysis showed that between the ages of 40 and 49 years, more than 60% of the survivor group had either pre-diabetes or diabetes.51 Dixon, S. B. et al. Prediabetes and Associated Risk of Cardiovascular Events and Chronic Kidney Disease Among Adult Survivors of Childhood Cancer in the St Jude Lifetime Cohort. Journal of Clinical Oncology 42, 1031–1043 (2024). https://doi.org/10.1200/jco.23.01005
- Overall, survivors treated with abdominopelvic radiotherapy treatment (ART) were three times more likely to develop a subsequent colorectal cancer (CRC) than those who did not receive ART.52 Heymer, E. J. et al. Cumulative Absolute Risk of Subsequent Colorectal Cancer After Abdominopelvic Radiotherapy Among Childhood Cancer Survivors: A PanCareSurFup Study. Journal of Clinical Oncology 42, 336–347 (2024). https://doi.org/10.1200/jco.23.00452 (https://www.cmaj.ca/content/cmaj/suppl/2024/03/05/196.9.E282.DC1/231358-res-4-at.pdf ) to monitor adults who had cancer as children.53 Shuldiner, J. et al. Longitudinal adherence to surveillance for late effects of cancer treatment: a population-based study of adult survivors of childhood cancer. Canadian Medical Association Journal 196, E282–E294 (2024). https://doi.org/10.1503/cmaj.231358
- The North American Children's Oncology Group has developed long-term follow-up guidelines(https://www.cmaj.ca/content/cmaj/suppl/2024/03/05/196.9.E282.DC1/231358-res-4-at.pdf ) to monitor adults who had cancer as children.54Shuldiner J, Sutradhar R, Lau C, et al. Longitudinal adherence to surveillance for late effects of cancer treatment: a population-based study of adult survivors of childhood cancer. Can Med Assoc J. 2024;196(9):E282-E294. doi:10.1503/cmaj.231358
- Childhood cancer survivors have more than a two-fold increased risk of melanoma compared with the general population, and those with an invasive melanoma have more than a two-fold risk of death.55 Rotz, S. J. et al. Melanoma Among Adult Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. Journal of Clinical Oncology 43, 1219–1228 (2025). https://doi.org/10.1200/jco-24-01519
- Compared to the general population, survivors of childhood cancer had a greater association with negative employment transition. There was an association between negative employment transition and chronic health conditions, and individuals with more chronic health conditions had worse transitions.56 Bhatt, N. S. et al. Chronic Health Conditions and Longitudinal Employment in Survivors of Childhood Cancer. JAMA Network Open 7, e2410731 (2024). https://doi.org/10.1001/jamanetworkopen.2024.10731
- Childhood cancer survivors have a persistent risk of subsequent leukemia beyond 10 years, especially with high epipodophyllotoxin exposure. Survivors show a 9-fold increased risk for late leukemia and a 5.9-fold risk for very late leukemia compared to the general population. Older age at primary diagnosis, cranial or total body irradiation, and hematopoietic cell transplantation increase leukemia risk.57 Ghosh, T. et al. Late subsequent leukemia after childhood cancer: A report from the Childhood Cancer Survivor Study (CCSS). Cancer Medicine 13 (2024). https://doi.org/10.1002/cam4.70086
- Childhood cancer survivors experience fear of recurrence even decades later. Overall, 16.6% of the survivors reported a clinically significant fear of cancer recurrence, and an additional 15.7% reported a high fear of cancer recurrence.58 Pizzo, A. et al. Fear of Cancer Recurrence in Adult Survivors of Childhood Cancer. JAMA Network Open 7, e2436144 (2024). https://doi.org/10.1001/jamanetworkopen.2024.36144
- Pediatric cancer survivors, particularly those with brain tumors or those who are diagnosed at a young age, face a higher risk of attention-deficit/hyperactivity disorder (ADHD) and increased use of ADHD medications. Chemotherapy administered to infants and toddlers significantly increases the risk of ADHD. Radiotherapy increases this risk in patients with ALL.59 Kim, J. S., Lee, J. & Lee, J. H. Attention-deficit/hyperactivity disorder in pediatric cancer survivors: risk and medication use in a nationwide population-based study. Child Adolesc Psychiatry Ment Health (2026). https://doi.org/10.1186/s13034-026-01062-z
- 23% of survivors of medulloblastoma developed posterior fossa syndrome. Compared with participants without posterior fossa syndrome, those with posterior fossa syndrome had significant deficits in attention, processing speed, and cognitive flexibility, and physical function.60 Sarvode, S. et al. Long-Term Outcomes Associated With Posterior Fossa Syndrome in Survivors of Childhood Medulloblastoma. JAMA Network Open 9, e2559376 (2026). https://doi.org/10.1001/jamanetworkopen.2025.59376
- Certain high-risk populations of childhood cancer survivors may be suitable candidates for screening for subsequent meningiomas. In a cohort study of survivors in the Childhood Cancer Survivor Study cohort, 471 survivors were diagnosed with 710 meningiomas; 35 after primary cancer diagnosis, the cumulative incidence of a subsequent meningioma was 2.3%. Meningioma risk was associated with high doses of radiation therapy, young age at primary cancer diagnosis, female sex, and exposure to platinum, antimetabolite chemotherapy, and intrathecal chemotherapy.61 Bowers, D. C. et al. Subsequent Meningiomas Among Survivors of Childhood Cancer. JAMA Network Open 8, e2548715 (2025). https://doi.org/10.1001/jamanetworkopen.2025.48715
- Adult survivors of childhood cancer have statistically significant accelerated brain aging (6.6 years older) compared with controls, which is associated with lower neurocognitive function and elevated biomarkers of oxidative stress, vascular health, and neuroinflammation. Female survivors who were treated with 40 Gy or higher cranial radiation before 10 years of age had the most evidence of brain aging.62 Phillips, N. S. et al. Accelerated Brain Aging, Atherogenicity, and Neurocognition in Adult Survivors of Childhood Cancer. JAMA Network Open 8, e2551865 (2025). https://doi.org/10.1001/jamanetworkopen.2025.51865
Factors Affecting Follow-up Care
The US Government Accountability Office (GAO) sought to identify factors reported to affect access to follow-up care for childhood cancer survivors. Stakeholders that the GAO interviewed and studies reviewed by the GAO identified three factors that affect access to follow-up care for childhood cancer survivors—individuals of any age who were diagnosed with cancer from ages 0 through 1963 Farb, J., Bozzolo, H., Buentello, M., Carlson, B. & Piercy, S. Survivors of Childhood Cancer: Factors Affecting Access to Follow-up Care. (US Government Accountability Office, 2022). :
Affordability: Survivors of childhood cancer may have difficulty paying for follow-up care, which can affect their access to this care. For example, one study found that survivors were significantly more likely to have difficulty paying medical bills and delay medical care due to affordability concerns when compared to individuals with no history of cancer.
Knowledge: Survivors’ access to appropriate follow-up care for late effects of childhood cancer can depend on both survivors’ and providers’ knowledge about such care, which can affect access in various ways, according to stakeholders GAO interviewed and studies GAO reviewed:
- Some survivors may have been treated for cancer at an early age and may have limited awareness of the need for follow- up care.
- Some primary or specialty care providers may not be knowledgeable about guidelines for appropriate follow-up care, which can affect whether a survivor receives recommended treatment. Follow-up care may include psychosocial care (e.g., counseling), and palliative care (e.g., pain management).
Proximity: Survivors may have difficulty reaching appropriate care settings. Stakeholders GAO interviewed and studies GAO reviewed noted that childhood cancer survivors may have to travel long distances to receive follow-up care from multidisciplinary outpatient clinics—referred to as childhood cancer survivorship clinics. The lack of proximity may make it particularly difficult for survivors with limited financial resources to adhere to recommended follow-up care.
Alarmingly, few childhood cancer survivors undergo recommended surveillance for late effects. Only about one-third of survivors adhered to monitoring recommendations for each late effect (cardiac, 36.1%; thyroid, 31.9%; breast, 36.4%).64 Milam, J., Kim, Y., Roth, M. & Freyer, D. R. Late effects surveillance adherence among young adult childhood cancer survivors: A population-based study. Pediatr Blood Cancer 71, e31328 (2024). <a href=”https://doi.org/10.1002/pbc.31328″ target=”_blank” rel=”noopener noreferrer”>https://doi.org/10.1002/pbc.31328</a>
Socioeconomic Impact of Pediatric Cancer
- On average, in 2009, pediatric hospitalizations principally for cancer were 8 days longer and cost nearly 5 times as much as hospitalizations for other conditions (12.0 days versus 3.8 days; $40,400 versus $8,100 per stay). Costs per day were about 70 percent higher for pediatric cancer stays ($3,900 versus $2,300 per day). Pediatric stays principally for cancer cost nearly one billion dollars, accounting for over 5 percent of pediatric non-newborn inpatient hospital costs.65 Price, R. A., Stranges, E. & Elixhauser, A. in Healthcare Cost and Utilization Project (HCUP) Statistical Briefs (2006).
- Among 469 parents of childhood cancer survivors surveyed (mean = 24 years after diagnosis), 21% reported employment changes: e.g., work time reduction (52%), quitting (27%), and taking unpaid leave (21%). Some parents reported professional (5%) or financial long-term impact (5%). Financial impact was mainly associated with survivors experiencing late effects, cancer relapse, or survivors’ financial dependence. Professional impact was associated with female sex and employment changes.66 Ospelt, M. et al. Parental employment adjustment during and after childhood cancer treatment — a report from the Swiss Childhood Cancer Survivor Study-Parents. Supportive Care in Cancer 33 (2025). https://doi.org/10.1007/s00520-025-09599-z
- Childhood cancer has a substantial impact on parents' socio-economic situation. Adverse socio-economic consequences were most pronounced shortly after diagnosis. They persisted into early survivorship for certain groups of parents. Families of children diagnosed with hematological cancers, younger age at diagnosis, and lower parental socio-economic position were significant risk factors for adverse socio-economic consequences.67 Roser, K., Erdmann, F., Michel, G., Winther, J. F. & Mader, L. The impact of childhood cancer on parents' socio-economic situation-A systematic review. Psychooncology 28, 1207–1226 (2019). https://doi.org/10.1002/pon.5088
- Parents of long-term childhood cancer survivors reported lower household income and a higher risk of poverty. In a study group of 383 parents of long-term childhood cancer survivors, 30.4% reported lower household income and were at a higher risk of poverty.68 Mader, L. et al. Household income and risk-of-poverty of parents of long-term childhood cancer survivors. Pediatr Blood Cancer 64 (2017). https://doi.org/10.1002/pbc.26456
- A 15-year trend for clinical trials on cellular therapy for children and adolescents (ages 0-19) with cancer in the US concluded that 169 (84%) of 202 trials posted 2007-2022 also included adult populations, only 3 trials enrolled children only. There was no industry funding for CNS tumors.69 Cho, S., Miller, A., Mosha, M., McNerney, K. O. & Metts, J. Clinical Trials on Cellular Therapy for Children and Adolescents With Cancer: A 15-Year Trend in the United States. Cureus 15, e47885 (2023). https://doi.org/10.7759/cureus.47885
- More than 90% of children and adolescents who are diagnosed with cancer each year in the United States are cared for at a children’s cancer center that is affiliated with the NCI-supported Children’s Oncology Group (COG). Children’s Oncology Group is the world’s largest organization that performs clinical research to improve the care and treatment of children and adolescents with cancer. Each year, approximately 4,000 children who are diagnosed with cancer enroll in a COG-sponsored clinical trial. COG trials are sometimes open to individuals aged 29 years or older when the type of cancer being studied is one that occurs in children, adolescents, and young adults.70 National Cancer Institute. Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15–39), https://seer.cancer.gov/statfacts/html/aya.html (2024).
- Lower area-level SES was significantly associated with worse overall survival in a cohort of children with ALL in the United States, an association that persisted when conditioned on surviving the first 2 years and 5 years from cancer diagnosis.71 Hoppmann, A. L. et al. Neighborhood socioeconomic status and overall survival among children with acute lymphoblastic leukemia. Blood Advances 9, 5861–5869 (2025). https://doi.org/10.1182/bloodadvances.2025017044
Funding
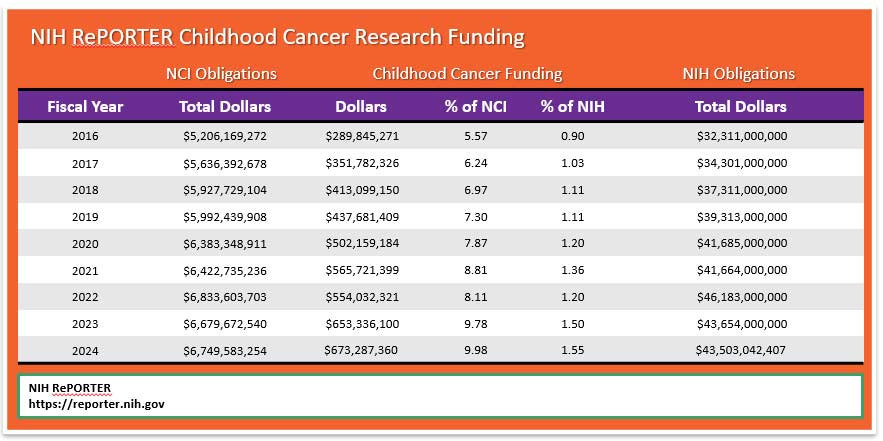
NCI uses the NIH RePORTER, which is a congressionally mandated system all NIH Institutes and Centers (ICs) used to report data by fiscal year (FY). This tool highlights annual support for various Research, Condition, and Disease Categories (RCDC) based on grants, contracts, and other funding mechanisms used across NIH. According to Office of Advocacy Relations, the NIH RePORTER does not account for the totality of NCI’s investment in a given area of research because basic science awards cannot be categorized by individual cancer type. Using Total NCI Obligations, without making allowances for NIH items included in the Pediatric Cancer Amount, would distort the percentage of Total Obligations.
Since we are unable to capture a completely accurate measure of childhood cancer research expenditure as it relates to total research dollars, perhaps a better method to measure progress may be to compare NIH RePORTER pediatric dollars (b) to the Total NIH Dollars (c) for each fiscal year. This method would show changes from one year to the next. Note that the chart below shows growth in pediatric cancer expenditures from 2016 to 2024.
Mortality
- Cancer is the second most common cause of death among children aged 1–14 years (after accidents) and the fourth most common cause of death (after accidents, homicide, and suicide) among adolescents (aged 15–19 years).72 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- On average, about 14% of children die within 5 years of diagnosis, among those children treated in the 70’s and 80’s who survived to five years from diagnosis, 18% of them will die over the next 25 years. In recent decades, cancer treatments have been modified with the goal of reducing life-threatening late effects.73 Armstrong, G. T. et al. Reduction in Late Mortality among 5-Year Survivors of Childhood Cancer. N Engl J Med 374, 833–842 (2016). https://doi.org/10.1056/NEJMoa1510795
- 1050 children (aged 0 -14) and 600 adolescents (aged 15-19) are expected to die from cancer in 2025.74 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- It is estimated that in 2023, there were 9,050 deaths due to cancer among AYAs aged 15 to 39.75 National Cancer Institute. Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15–39), https://seer.cancer.gov/statfacts/html/aya.html (2024).
- Cancer mortality has declined steadily since 1970, from 6.3 to 1.9 per 100,000 in 2020–2022 in children and from 7.2 to 2.7 in adolescents, for overall reductions of 70% and 63%, respectively.76 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- The 5-year relative survival rate for all cancers combined improved from 58% for diagnoses during the mid-1970s to 85% during 2014 through 2020 in children and from 68% to 87% in adolescents, but it varies substantially by cancer type and age at diagnosis.77 Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H. & Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians 75, 10–45 (2025). https://doi.org/10.3322/caac.21871
- Between 2015 and 2019, cancer death rates decreased an average of 1.5% per year among children ages 0 to 14, while death rates for AYAs (ages 15 to 39) decreased an average of 0.9% per year.78 Cronin, K. A. et al. Annual report to the nation on the status of cancer, part 1: National cancer statistics. Cancer 128, 4251–4284 (2022). https://doi.org/10.1002/cncr.34479
- Brain cancer represents 25% of total childhood cancer deaths, while leukemia accounts for 28%.79 Siegel, R. L., Giaquinto, A. N. & Jemal, A. Cancer statistics, 2024. CA Cancer J Clin 74, 12–49 (2024). https://doi.org/10.3322/caac.21820
- The median age at death for childhood brain and CNS cancers is age 9.80 National Cancer Institute. Cancer Stat Facts: Childhood Brain and Other Nervous System Cancer (Ages 0–19), https://seer.cancer.gov/statfacts/html/childbrain.html (2024).
- Pediatric brain and other central nervous system tumors are the leading cause of cancer-related fatalities in children and adolescents aged birth to 19 years old. Improvements in mortality in pediatric and adolescent primary central nervous system (CNS) malignancies have lagged behind those of other cancers.81 Rumberger Rivera, L. et al. Opportunities in the translational pipeline for pediatric brain cancer therapies. Pediatric Research 98, 800–806 (2025). https://doi.org/10.1038/s41390-025-03847-y
- Suicide rates rose for individuals with cancer over the past 20-plus years. Rates of death by suicide per 1000 increased the most among adolescent and young adult men from 4.9 in 2000 to 15.4 in 2021. Deaths by suicide often occurred years after cancer diagnosis — particularly for AYAs (age 15 to 39 years) with thyroid cancer (36.6 per 1,000), testicular cancer (36.3 per 1,000), or melanoma (24.4 per 1,000).82 Matsuo, K. et al. Suicide Deaths Among Adolescent and Young Adult Patients With Cancer. JAMA Netw Open 7, e2442964 (2024). https://doi.org/10.1001/jamanetworkopen.2024.42964
- More than half of children with cancer die in the hospital. Researchers from multiple institutions analyzed trends in the place of death for children diagnosed with cancer between 2003 and 2020. About half (52%) died in the hospital, 39.3% died at home, 6.1% died in outpatient medical facilities, 2.2% died in hospice, and 0.5% died in nursing facilities.83 Jain, U. et al. Trends in Location of Death for Individuals With Pediatric Cancer. JAMA Pediatr 178, 1221–1223 (2024). https://doi.org/10.1001/jamapediatrics.2024.3102
- Those that survive the five years have an eight times greater mortality rate due to the increased risk of liver and heart disease, and increased risk for reoccurrence of the original cancer or of a secondary cancer.84 Mertens, A. C. et al. Cause-specific late mortality among 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study. J Natl Cancer Inst 100, 1368–1379 (2008). https://doi.org/10.1093/jnci/djn310
- There are 69.3 potential life years lost on average when a child dies of cancer 85 Stat bite: Average years of life lost from cancer. J Natl Cancer Inst 93, 341 (2001). https://doi.org/10.1093/jnci/93.5.341 compared to 12 potential life years lost for adults.86 Arias, E., Kochanek, K., Xu, J. & Tajeda-Vera, B. Provisional Life Expectancy Estimates for 2022. (National Center for Health Statistics, 2023).
- Survivors of hereditary retinoblastoma, a rare cancer of the eye, have a high risk of developing subsequent cancers, particularly sarcomas of the soft tissue and bone.87 Schonfeld, S. J. et al. Long-term risk of subsequent cancer incidence among hereditary and nonhereditary retinoblastoma survivors. Br J Cancer 124, 1312–1319 (2021). https://doi.org/10.1038/s41416-020-01248-y
- Despite improvements in 5-year survival, long-term survivors of childhood cancer are at four times the risk of death compared with the general, aging population.88 Dixon, S. B. et al. Specific causes of excess late mortality and association with modifiable risk factors among survivors of childhood cancer: a report from the Childhood Cancer Survivor Study cohort. Lancet 401, 1447–1457 (2023). https://doi.org/10.1016/S0140-6736(22)02471-0
Drug Development
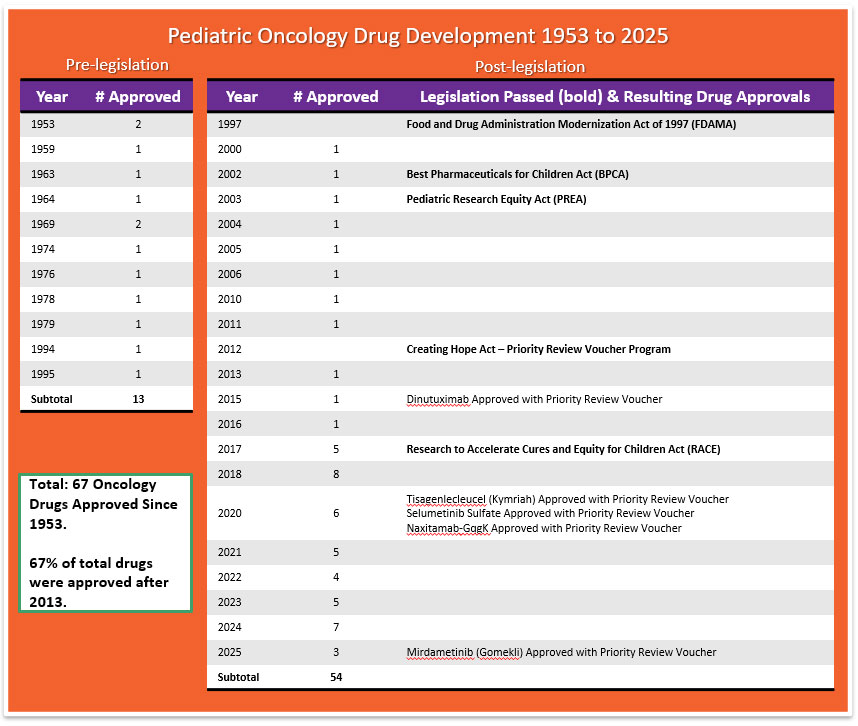
- The FDA awarded Priority Review Vouchers (PRV) for four of the seven drugs originally approved in the first instance for cancer treatment for children. PRV’s are transferable and are desired incentives for developers of drugs for rare pediatric diseases. Holders of a PRV get a faster FDA drug approval process for a future drug of their choice. The vouchers are transferable and may be sold or traded.89 Office of Orphan Products Development. Rare Pediatric Disease Designation and Priority Review Voucher Programs, https://www.fda.gov/industry/medical-products-rare-diseases-and-conditions/rare-pediatric-disease-designation-and-priority-review-voucher-programs (2024).
- The US Congress created the priority review voucher program in 2007 based on a 2006 Health Affairs paper (Ridley et al. 2006). The voucher entitles the bearer to regulatory review in about six months rather than the standard ten months. The Food and Drug Administration (FDA) awards a voucher following approval of a treatment for a neglected disease, rare pediatric disease (Cancer is included in rare pediatric disease) or medical countermeasure. Two drugs receive priority review for each voucher: the drug winning a voucher for a neglected or rare pediatric disease and the drug using a voucher for another indication. The voucher may be sold. For example, a small company might win a voucher for developing a drug for a neglected disease and sell the voucher to a large company for use on a commercial disease. Vouchers can sell for 100’s of millions of dollars.90 Ridley, D. Priority Review Vouchers, https://sites.fuqua.duke.edu/priorityreviewvoucher/ (2026).
- While more than 200 cancer drugs have been developed and approved for adults,91 Cronin, K. A. et al. Annual report to the nation on the status of cancer, part 1: National cancer statistics. Cancer 128, 4251–4284 (2022). https://doi.org/10.1002/cncr.34479 the FDA through December, 2025 has approved a total of 67 drugs for use in the treatment of childhood cancers. Today we have eight drugs that were approved in the first instance for use in cancer treatment for children: Teniposide (1992 for ALL) use now discontinued by NCI, clofarabine (2004 for ALL), dinutuximab (2015 for NB), tisagenlecleucel (2017 for ALL), calaspargase pegol-mk (2018 for ALL), selumetinib (2020 for NF1), naxitamab (2020 for NB), eflornithine (2023 for HRNB), mirdametinib (2025 for NF1).92 National Cancer Institute. Drugs Approved for Childhood Cancers, https://www.cancer.gov/about-cancer/treatment/drugs/childhood-cancer-fda-approved-drugs (2025). In addition, the FDA has approved 8 drugs that help to reduce the toxicity associated with certain cancer treatments.93 Biltaji, E. et al. Supportive care medications coinciding with chemotherapy among children with hematologic malignancy. Leuk Lymphoma 61, 1920–1931 (2020). https://doi.org/10.1080/10428194.2020.1749604
- The median lag time from first-in-human to first-in-child trials of oncology agents that were ultimately approved by FDA was 6.5 years.94 Neel, D. V., Shulman, D. S. & DuBois, S. G. Timing of first-in-child trials of FDA-approved oncology drugs. Eur J Cancer 112, 49–56 (2019). https://doi.org/10.1016/j.ejca.2019.02.011
- Between the years of 2009 and 2019, nine of the 11 drugs used to treat acute lymphoblastic leukemia — which is the most common childhood cancer — were in and out of shortage.95 U.S. Food and Drug Association. Drug Shortages: Root Causes and Potential Solutions. (Drug Shortages Task Force, 2020).
- Researchers found that the probability of FDA drug approval within 10 years was 10.4%, and the probability that development would stall within 10 years was 49.2%.96 Arfe, A., Narang, C., DuBois, S. G., Reaman, G. & Bourgeois, F. T. Clinical development of new drugs for adults and children with cancer, 2010-2020. J Natl Cancer Inst 115, 917–925 (2023). https://doi.org/10.1093/jnci/djad082
Global Facts
- Global 5-year net childhood cancer survival is currently estimated at 37.4%.97 Ward, Z. J. et al. Global childhood cancer survival estimates and priority-setting: a simulation-based analysis. Lancet Oncol 20, 972–983 (2019). https://doi.org/10.1016/S1470-2045(19)30273-6
- In 2017, childhood cancer was the sixth leading cause of total cancer burden globally and the ninth leading cause of childhood disease burden globally.98 Stiller, C. A. Global burden of childhood cancer: growing, but controllable. Lancet Oncol 20, 1184–1185 (2019). https://doi.org/10.1016/S1470-2045(19)30424-3
- Approximately 80% of pediatric tumors occur in low- and middle-income countries (LMIC), where diagnostic tools essential for treatment decisions are often unavailable or incomplete.99 Opoku, K. B. et al. Transcriptome profiling of pediatric extracranial solid tumors and lymphomas enables rapid low-cost diagnostic classification. Sci Rep 14, 19456 (2024). https://doi.org/10.1038/s41598-024-70541-0
- Approximately 90% of children with cancer live in low-income and middle-income countries (LMICs), where 5-year survival is lower than 20%.100 Ehrlich, B. S. et al. Treatment-related mortality in children with cancer in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Oncol 24, 967–977 (2023). https://doi.org/10.1016/S1470-2045(23)00318-2
- Approximately 1 in 15 children receiving cancer treatment in low- and middle-income countries die from treatment-related complications. Although treatment-related mortality has decreased in upper–middle-income countries over time, it remains unchanged in low- and middle-income countries.101 Ehrlich, B. S. et al. Treatment-related mortality in children with cancer in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Oncol 24, 967–977 (2023). https://doi.org/10.1016/S1470-2045(23)00318-2
- In 2019, cancer was the fourth leading cause of death and tenth leading cause of Disability-Adjusted Life Years (DALYs) in adolescents and young adults (ages 15 to 39) globally.102 Collaborators, G. B. D. A. Y. A. C. The global burden of adolescent and young adult cancer in 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Oncol 23, 27–52 (2022). https://doi.org/10.1016/S1470-2045(21)00581-7
- When the overall disease burden is studied within the age range encompassing adolescents and young adults (aged 15 years to 39 years), the global burden of cancer contributed more Disability-Adjusted Life Years (DALYs), a combination of Years of Life Lost (YLLs) and Years Lived with Disability (YLDs), to the global disease burden than some high-profile communicable diseases such as HIV/AIDS and sexually transmitted infections.103 Collaborators, G. B. D. A. Y. A. C. The global burden of adolescent and young adult cancer in 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Oncol 23, 27–52 (2022). https://doi.org/10.1016/S1470-2045(21)00581-7
- In 2019, 43% (172,000 of 397,000) of childhood cancer cases were undiagnosed globally.104 Ward, Z. J., Yeh, J. M., Bhakta, N., Frazier, A. L. & Atun, R. Estimating the total incidence of global childhood cancer: a simulation-based analysis. Lancet Oncol 20, 483–493 (2019). https://doi.org/10.1016/S1470-2045(18)30909-4
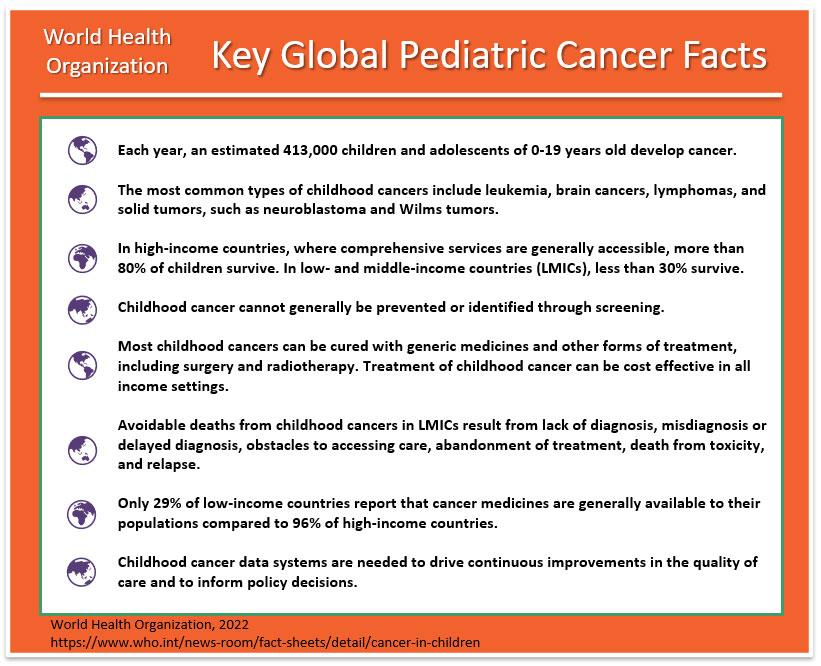
- Cancer kills more than 100,000 children (birth to 19) each year, and yet 80% of pediatric cancers are curable with currently available interventions. Notably, the majority of these deaths occur in low‐income and middle-income countries where children have poor access to health services.105 Atun, R. et al. Sustainable care for children with cancer: a Lancet Oncology Commission. The Lancet Oncology 21, e185–e224 (2020). https://doi.org/10.1016/s1470-2045(20)30022-x
- In Europe, since 1995, a total of 16 drugs have been approved for pediatric cancers. Seven of the 16 have been approved in the first instance specifically for pediatric cancers. Nine of the 16 were first approved for adults, then later for use in pediatric cancer. Eight of the total 16 drugs affected cancers responsible for less than 6% of all European childhood cancer deaths.106 Vassal, G., de Rojas, T. & Pearson, A. D. J. Impact of the EU Paediatric Medicine Regulation on new anti-cancer medicines for the treatment of children and adolescents. Lancet Child Adolesc Health 7, 214–222 (2023). https://doi.org/10.1016/S2352-4642(22)00344-3
- In Europe, cancer is diagnosed in 1 in 350 children before age 15 years and is the leading disease-related cause of death in childhood after infancy.107 Soegaard, S. H. et al. Exclusive Breastfeeding Duration and Risk of Childhood Cancers. JAMA Netw Open 7, e243115 (2024). https://doi.org/10.1001/jamanetworkopen.2024.3115
- In 2018, The World Health Organization (WHO) launched the Global Initiative for Childhood Cancer with partners to provide leadership and technical assistance to support governments in building and sustaining high-quality childhood cancer programs. The goal is to achieve at least 60% survival rate globally by 2030, for all children with cancer. This represents an approximate doubling of the current cure rate and will save an additional one million lives over the next decade. The objectives are to increase capacity of countries to deliver best practices in childhood cancer care and also to prioritize childhood cancer and increase available funding at the national and global levels.108 World Health Organization. Childhood cancer, https://www.who.int/news-room/fact-sheets/detail/cancer-in-children (2025).
- Some cancers are more prevalent in developing countries. For example, Burkitt’s lymphoma is more common in East and West Africa with over 4,000 cases in East Africa and over 10,000 in West Africa while only around 20 were recorded in the UK in 2015.109 World Health Organization. Childhood cancer, https://www.who.int/news-room/fact-sheets/detail/cancer-in-children (2025).
- Because most of the world's population is NOT covered by cancer surveillance systems or vital registration found in developed countries, and in addition, childhood cancer is rare and often presents with non-specific symptoms that mimic those of more prevalent infectious and nutritional conditions found in many low-income developing countries. Worldwide/UN-regional cancer incidence is therefore estimated using a Baseline Model (BM) method to quantify the cancer burden in children. It is estimated that there will be 13.7 million cases of childhood cancer between 2020-2050. Unless there are major improvements in diagnosis and treatments, of this, 45% will go undiagnosed and 11.1 million will die if no further investments in interventions are made. The vast majority, almost 85%, will be concentrated in developing countries.110 Atun, R. et al. Sustainable care for children with cancer: a Lancet Oncology Commission. The Lancet Oncology 21, e185–e224 (2020). https://doi.org/10.1016/s1470-2045(20)30022-x
- Current projections show that Africa will account for nearly 50% of the global childhood cancer burden by 2050.111 Moeti, M. World Cancer Day 2023, https://www.afro.who.int/regional-director/speeches-messages/world-cancer-day-2023 (2023).
- Survival was higher in registries included from the Caribbean and Central America, Asia, and the Middle East and North Africa compared with those included from South America and sub-Saharan Africa. Survival correlated with the Human Development Index. For leukemia, 3-year survival varied from 30.4% in Kenya to 89.5% in Puerto Rico; for central nervous system tumors from 32.0% in Algeria to 79.3% in Puerto Rico.112 Daltveit, D. S. et al. Childhood cancer survival in Africa, Asia, Latin America and the Caribbean, during 2008-2017 (SURVCAN-3): a population-based benchmarking study of 16 821 children. JNCI: Journal of the National Cancer Institute (2025). https://doi.org/10.1093/jnci/djaf321
Psychosocial Care
Note: Psychosocial care addresses the effects that cancer treatment has on the mental health and emotional wellbeing of patients, their family members, and their professional caregivers. A single profession alone does not provide psychosocial care: Instead, every patient-healthcare provider interaction provides an opportunity to assess the stressors and concerns of children and their family members.
- The provision of psychosocial care has been shown to yield better management of common disease-related symptoms and adverse effects of treatment, such as pain and fatigue.113 Jacobsen, P. B., Holland, J. C. & Steensma, D. P. Caring for the whole patient: the science of psychosocial care. J Clin Oncol 30, 1151–1153 (2012). https://doi.org/10.1200/JCO.2011.41.4078
- For children and families, treating the pain, symptoms, and stress of cancer enhances quality of life and is as important as treating the disease.114 in Comprehensive Cancer Care for Children and Their Families: Summary of a Joint Workshop by the Institute of Medicine and the American Cancer Society The National Academies Collection: Reports funded by National Institutes of Health (2015).
- Childhood cancer survivors reported higher rates of pain, fatigue, and sleep difficulties compared with siblings and peers, all of which are associated with poorer quality of life.115 Armenian, S. H. et al. Children's Oncology Group's 2013 blueprint for research: survivorship and outcomes. Pediatr Blood Cancer 60, 1063–1068 (2013). https://doi.org/10.1002/pbc.24422
- Changes in routines disrupt the day-to-day functioning of siblings.116 Zegaczewski, T., Chang, K., Coddington, J. & Berg, A. Factors Related to Healthy Siblings' Psychosocial Adjustment to Children With Cancer: An Integrative Review. J Pediatr Oncol Nurs 33, 218–227 (2016). https://doi.org/10.1177/1043454215600426 Siblings of children with cancer are at risk for emotional and behavioral difficulties, such as anxiety, depression, and post-traumatic stress disorder.117 Kaplan, L. M., Kaal, K. J., Bradley, L. & Alderfer, M. A. Cancer-related traumatic stress reactions in siblings of children with cancer. Fam Syst Health 31, 205–217 (2013). https://doi.org/10.1037/a0032550
- Symptoms of posttraumatic stress disorder are well documented for parents whose children have completed cancer treatment.118 Kazak, A. E. et al. Posttraumatic stress disorder (PTSD) and posttraumatic stress symptoms (PTSS) in families of adolescent childhood cancer survivors. J Pediatr Psychol 29, 211–219 (2004). https://doi.org/10.1093/jpepsy/jsh022
- Chronic grief has been associated with many psychological (e.g., depression and anxiety) and somatic symptoms (e.g., loss of appetite, sleep disturbances, fatigue), including increased mortality risk.119 Alam, R., Barrera, M., D'Agostino, N., Nicholas, D. B. & Schneiderman, G. Bereavement experiences of mothers and fathers over time after the death of a child due to cancer. Death Stud 36, 1–22 (2012). https://doi.org/10.1080/07481187.2011.553312
- Financial hardship during childhood cancer has been found to affect a significant proportion of the population and to negatively impact family well-being.120 Bona, K. et al. Economic impact of advanced pediatric cancer on families. J Pain Symptom Manage 47, 594–603 (2014). https://doi.org/10.1016/j.jpainsymman.2013.04.003
- Adolescents with cancer experienced significantly more Health Related Hindrance (HRH) of personal goals than healthy peers, and their HRH was significantly associated with poorer health-related quality of life, negative affect, and depressive symptoms.121 Schwartz, L. A. & Brumley, L. D. What a Pain: The Impact of Physical Symptoms and Health Management on Pursuit of Personal Goals Among Adolescents with Cancer. J Adolesc Young Adult Oncol 6, 142–149 (2017). https://doi.org/10.1089/jayao.2016.0031
- Chronic health conditions resulting from childhood cancer therapies contribute to emotional distress in adult survivors.122 Vuotto, S. C. et al. Impact of chronic disease on emotional distress in adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 123, 521–528 (2017). https://doi.org/10.1002/cncr.30348
- Parents have been found to report significant worsening of all their own health behaviors, including poorer diet and nutrition, decreased physical activity, and less time spent engaged in enjoyable activities 6 to 18 months following their child’s diagnosis.123 Wiener, L. et al. Impact of Caregiving for a Child With Cancer on Parental Health Behaviors, Relationship Quality, and Spiritual Faith: Do Lone Parents Fare Worse? J Pediatr Oncol Nurs 33, 378–386 (2016). https://doi.org/10.1177/1043454215616610
Prevention
- Any substance that causes cancer is known as a carcinogen. But simply because a substance has been designated as a carcinogen does not mean that the substance will necessarily cause cancer. Many factors influence whether a person exposed to a carcinogen will develop cancer, including the amount and duration of the exposure and the individual’s genetic background.124 National Cancer Institute. Environmental Carcinogens and Cancer Risk, https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/carcinogens (2023).
- Cancers caused by involuntary exposures to environmental carcinogens are most likely to occur in subgroups of the population, such as workers in certain industries who may be exposed to carcinogens on the job.125 National Cancer Institute. Environmental Carcinogens and Cancer Risk, https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/carcinogens (2023).
- Two organizations—the National Toxicology Program (NTP), an interagency program of the U.S. Department of Health and Human Services (HHS), and the International Agency for Research on Cancer (IARC), the cancer agency of the World Health Organization—have developed lists of substances that, based on the available scientific evidence, are known or are reasonably anticipated to be human carcinogens.126 National Cancer Institute. Environmental Carcinogens and Cancer Risk, https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/carcinogens (2023).
- The National Toxicology Program (NTP) cumulative report now includes 256 listings of substances — chemical, physical, and biological agents; mixtures; and exposure circumstances — that are known or reasonably anticipated to cause cancer in humans. The latest report, the 15th Report on Carcinogens was released on December 21, 2021.127 National Toxicology Program. 15th Report on Carcinogens. Rep Carcinog 15 (2021). https://doi.org/10.22427/NTP-OTHER-1003
- Childhood cancer is fundamentally different from adult cancer in its biology, clinical classification, and treatment. Most childhood cancers are not caused by modifiable risk factors, and public health campaigns would not have a large effect on decreasing their incidence.128 Valery, P. C. & McBride, C. A. Sustainable care for indigenous children with cancer. Lancet Oncol 21, 489–491 (2020). https://doi.org/10.1016/S1470-2045(20)30137-6
- Over the past 50 years, the use of artificial chemicals in products has increased exponentially. Most of these chemicals were not tested for safety before widespread use, and the impacts of exposures are just now being realized. Children are especially vulnerable to the health impacts of chemical exposures, and these exposures are now known to be an important component of rising rates of diseases such as asthma, some cancers, and neurodevelopmental disorders in children.129 Huffling, K. & McLaughlin, J. Pediatric Chemical Exposure: Opportunities for Prevention. J Pediatr Health Care 36, 27–33 (2022). https://doi.org/10.1016/j.pedhc.2021.09.009
- Children are at an elevated risk for chronic disease because of increased exposure to environmental toxins. The U.S. Environmental Protection Agency (EPA) (2017) identifies children as uniquely vulnerable to environmental risks because of rapidly developing brains, lungs, immune and other bodily systems with less developed natural defenses than adults, including more permeable blood-brain barriers, and metabolic and detoxification pathways that are not yet fully developed.130 Huffling, K. & McLaughlin, J. Pediatric Chemical Exposure: Opportunities for Prevention. J Pediatr Health Care 36, 27–33 (2022). https://doi.org/10.1016/j.pedhc.2021.09.009
- Phthalates are a class of chemicals found in a variety of products. They are mixed with polyvinyl chloride and other plastics as a plasticizer that helps to make them soft and flexible. They are also added to cosmetics and other personal care products (often as a fragrance stabilizer), in medical equipment and coatings on medications, food production equipment and packaging, flooring, wall coverings, and other home products.131 Huffling, K. & McLaughlin, J. Pediatric Chemical Exposure: Opportunities for Prevention. J Pediatr Health Care 36, 27–33 (2022). https://doi.org/10.1016/j.pedhc.2021.09.009 In a study of 1.3 million children aged under 19 years of age, childhood phthalate exposure was associated with incidence of osteosarcoma and lymphoma.132 Ahern, T. P. et al. Medication-Associated Phthalate Exposure and Childhood Cancer Incidence. J Natl Cancer Inst 114, 885–894 (2022). https://doi.org/10.1093/jnci/djac045
- Pesticides are a group of chemicals intended to kill unwanted insects, plants, molds, and rodents, making them inherently toxic chemicals. Pesticides are not species-specific in their neurotoxic properties—a wanted effect on the nervous system of an insect can also be an unwanted effect on the nervous system of a child.133 Huffling, K. & McLaughlin, J. Pediatric Chemical Exposure: Opportunities for Prevention. J Pediatr Health Care 36, 27–33 (2022). https://doi.org/10.1016/j.pedhc.2021.09.009 Exposures to pesticides, tobacco smoke, solvents, and traffic emissions have consistently demonstrated positive associations with risk of developing childhood leukemia.134 Whitehead, T. P., Metayer, C., Wiemels, J. L., Singer, A. W. & Miller, M. D. Childhood Leukemia and Primary Prevention. Curr Probl Pediatr Adolesc Health Care 46, 317–352 (2016). https://doi.org/10.1016/j.cppeds.2016.08.004
- Researchers found a higher level of common household pesticides in the urine of children with acute lymphoblastic leukemia. The findings should not be seen as cause-and-effect but suggest an association between pesticide exposure and the development of childhood ALL.135 Soldin, O. P. et al. Pediatric acute lymphoblastic leukemia and exposure to pesticides. Ther Drug Monit 31, 495–501 (2009). https://doi.org/10.1097/FTD.0b013e3181aae982
- The U.S. Environmental Protection Agency (EPA) reports that 75 percent of U.S. households used at least one pesticide product indoors during the past year. The EPA also states, “Exposure to pesticides may result in irritation to the eye, nose, and throat, damage to the central nervous system, the kidneys, and an increased risk of cancer.”136 Environmental Protection Agency. Pesticides' Impact on Indoor Air Quality, https://www.epa.gov/indoor-air-quality-iaq/pesticides-impact-indoor-air-quality (2025).
- Exposure to toxic substances, such as industrial chemicals and radiation, can increase the risk of leukemia. People may be exposed to radiation during imaging tests such as MRI, X-ray, and CT scans.137 Schmidt, J. A. et al. Risk Factors for Childhood Leukemia: Radiation and Beyond. Front Public Health 9, 805757 (2021). https://doi.org/10.3389/fpubh.2021.805757
- Since children are more radiosensitive than adults, and although CT scans are very useful clinically, potential cancer risks exist from associated ionizing radiation.138 Pearce, M. S. et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 380, 499–505 (2012). https://doi.org/10.1016/S0140-6736(12)60815-0
- Exposure of parents to ionizing radiation is also a possible concern in terms of the development of cancer in their future offspring. Children whose mothers had X-rays during pregnancy (that is, children who were exposed before birth) and children exposed after birth to diagnostic medical radiation from computed tomography (CT) scans have been found to have a slight increase in risk of leukemia, brain tumors, and possible other cancers.139 National Cancer Institute. Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15–39), https://seer.cancer.gov/statfacts/html/aya.html (2024).
- Risk of childhood leukemia was associated with higher crop area near mothers’ homes during pregnancy; CNS tumors were associated with higher cattle density.140 Patel, D. M. et al. Residential proximity to agriculture and risk of childhood leukemia and central nervous system tumors in the Danish national birth cohort. Environ Int 143, 105955 (2020). https://doi.org/10.1016/j.envint.2020.105955
- Intake of vitamins and folate supplementation during the preconception period or pregnancy has been demonstrated to have a protective effect.141 Metayer, C., Dahl, G., Wiemels, J. & Miller, M. Childhood Leukemia: A Preventable Disease. Pediatrics 138, S45–S55 (2016). https://doi.org/10.1542/peds.2015-4268H
- Researchers used statistical modeling to look at radon levels and cancer in 727 counties around the United States. Even at concentrations below the levels at which federal officials recommend steps to reduce radon exposure, they found links between childhood leukemia and radon. The U.S. Environmental Protection Agency says no level of radon is safe and recommends mitigation efforts when concentrations reach 148 Becquerels per cubic meter of air.142 Bozigar, M. et al. Domestic radon exposure and childhood cancer risk by site and sex in 727 counties in the United States, 2001-2018. Sci Total Environ 954, 176288 (2024). https://doi.org/10.1016/j.scitotenv.2024.176288
Disclaimer
THIS DOCUMENT IS NOT INTENDED TO OFFER SPECIFIC STATISTICS REGARDING AN INDIVIDUAL PATIENT OR THE PATIENT’S SPECIFIC FORM OF CANCER AND IS NOT A SUBSTITUTE FOR INFORMATION THAT MAY BE SOUGHT FROM A PHYSICIAN. IT IS MERELY INTENDED, BASED ON INFORMATION PRESENTLY AVAILABLE TO THE AUTHORS, TO BE A GOOD FAITH GENERAL PRESENTATION OF CHILDHOOD CANCER STATISTICS THAT MAY BE HELPFUL TO OTHERS SEEKING SUCH GENERAL INFORMATION.